

 Ask Prof. Hegab
Ask Prof. Hegab +201004401598
+201004401598
Facial trauma (Maxillo-facial trauma) is any physical trauma to the face. Facial trauma can involve soft tissue injuries such as burns, lacerations (cuts) and bruises or fractures (breaks) of the facial bones such as nasal fractures and fractures of the jaw, as well as trauma such as eye injuries.
 .
.
Pan Oro-Facial Trauma
Most maxillo-facial injuries are due to inter-personal violence and the majority are in previously fit young men (between 15 and 35 years of age); alcohol or another drug is frequently a factor.
The mandible (lower jaw) is twice as likely to be affected than the maxilla (upper jaw).
Road Traffic Accidents (RTA‘s) are also a major cause and produce fractures that often involve the mid-face, especially in patients who were not wearing seat-belts.
Industrial accidents, sports and epilepsy are other causes. Other important sources of facial trauma include abuse (children and older individuals).
High-impact maxillo-facial fractures often are associated with head and other bodily injuries that may be life-threatening. Patients are often multiply-injured and may have hazards to the airway, head, cervical (neck) or thoraco-lumbar spine, eye, chest, liver, spleen, kidneys, long bones or bladder and severe h?morrhage from massive mid-face injuries.
Extensive soft-tissue injuries or avulsions and comminuted fractures are difficult to treat and may have poor outcomes.
Low-impact maxillofacial fractures rarely result in mortality if proper treatment is administered.
Maxillofacial trauma demands special attention, since it may damage specialised functions, including breathing, sight, hearing, smelling, eating and speech – especially in middle third facial fractures (particularly Le Fort III fractures). The psychological impact of disfigurement can be devastating and vital structures in the head and neck region are intimately associated.
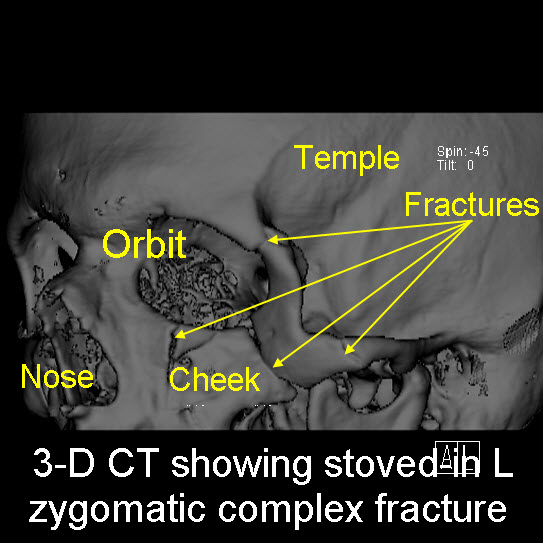
The bones most commonly fractured are the nasal, zygoma (cheek), mandible (lower jaw) and maxilla (upper jaw).
Many fractures are reduced and fixed with mini-plates and / or inter-maxillary fixation [link to Archbar Removal page].
Symptoms are specific to the type of injury; for example, fractures may involve pain, swelling, loss of function, or changes in the shape of facial structures.
Facial injuries have the potential to cause facial disfigurement and loss of function; for example, blindness or difficulty moving the jaw can result. Although it is seldom life-threatening, facial trauma has the potential to be fatal as it can cause severe bleeding or interference with the airway; thus a primary concern in treatment is ensuring that the airway is kept open and not threatened so that the patient can breathe.
Depending on the type of facial injury, treatment may include sewing up (suturing) of open wounds, administration of ice (to reduce swelling and bruising), antibiotics and pain killers, moving bones back into their correct position (manipulation) and surgery (reduction and fixation).
Where facial fractures are suspected, X-rays & CT scans are used for and to aid diagnosis.
Treatment may also be necessary for other injuries such as traumatic brain injury which commonly accompany facial trauma.
In developed countries, the leading cause of facial trauma is inter-personal violence; car accidents predominate as the main cause in developing countries and are still a major cause elsewhere. Other causes of facial trauma include falls, industrial accidents and sports injuries.
Epidemiology
Facial fractures are distributed in a fairly ‘normal’ curve by age, with a peak incidence occurring between ages 20 and 40 and children under 12 suffering only 5 – 10% of all facial fractures.
Most facial trauma in children involves lacerations and soft tissue injuries.
There are several reasons for the lower incidence of facial fractures in children:
- the face is smaller in relation to the rest of the head
- children are less often in those situations associated with facial fractures such as occupational and motor vehicle hazards
- the bone is differently proportioned in children making them more resistant to fracture
- poorly developed sinuses make the bones stronger, and
- fat pads provide protection for the facial bones.
